1. The Exercise Paradox: Introduction
For those living with fibromyalgia, medical advice often feels like a cruel contradiction. Clinical guidelines consistently point to exercise as the "first-line intervention"—the very thing most likely to improve long-term function and quality of life. Yet, for many, the act of moving triggers the very symptoms they are trying to escape. This creates a frustrating cycle: you are told to move to feel better, but movement makes you feel worse, leading to poor adherence and a decline in physical health.
As a physical therapist, I’ve seen this "Exercise Paradox" play out in clinics for years. Patients want to be active, but their nervous system punishes the attempt. However, results from a major new pragmatic clinical trial, known as the FM-TIPS study, suggest we have found a safe, accessible tool to bridge this gap. By targeting the pain that specifically occurs during activity, researchers have identified a way to make movement not just possible, but sustainable.
2. The Barrier We’ve Been Ignoring: Movement-Evoked Pain
While much of the research into fibromyalgia focuses on "resting pain"—the baseline ache that exists even while sedentary—the FM-TIPS study focused on a more functional obstacle: movement-evoked pain. This is the sharp increase in discomfort that occurs specifically during physical activity. In this study, researchers measured this barrier using the "5-times sit-and-stand task," a concrete metric that mirrors the real-world struggle of simply getting out of a chair.
When movement is consistently met with a spike in pain, the brain develops neural protective bracing and fear-avoidance behaviors. The nervous system essentially learns to "lock down" the body to prevent perceived injury. As the study authors emphasize:
"Fibromyalgia is characterized by chronic widespread pain that is often exacerbated by movement that interferes with daily activities."
To successfully treat fibromyalgia, we must do more than manage resting symptoms; we must dampen the pain during activity to show the nervous system that movement is safe.
3. TENS: Not Just a Lab Success, but a Real-World Solution
The study utilized Transcutaneous Electrical Nerve Stimulation (TENS), a method of delivering mild electrical pulses through the skin. Mechanically, TENS is fascinating: it activates endogenous inhibitory mechanisms in the central nervous system that "turn down the volume" of a sensitized system by reducing central excitability.
What makes the FM-TIPS trial so significant is its "pragmatic" design. Unlike traditional "ivory tower" studies conducted in sterile laboratories, this trial was embedded within 28 routine outpatient physical therapy clinics across six different health systems. It included 384 participants (91% female, mean age of 53) and was administered by local clinicians in the middle of their daily schedules. Because these results survived the "messiness" of real clinical practice, they are exceptionally relevant to the average person seeking care at their local clinic.
4. The 30% Threshold: Significant Relief for "Responders"
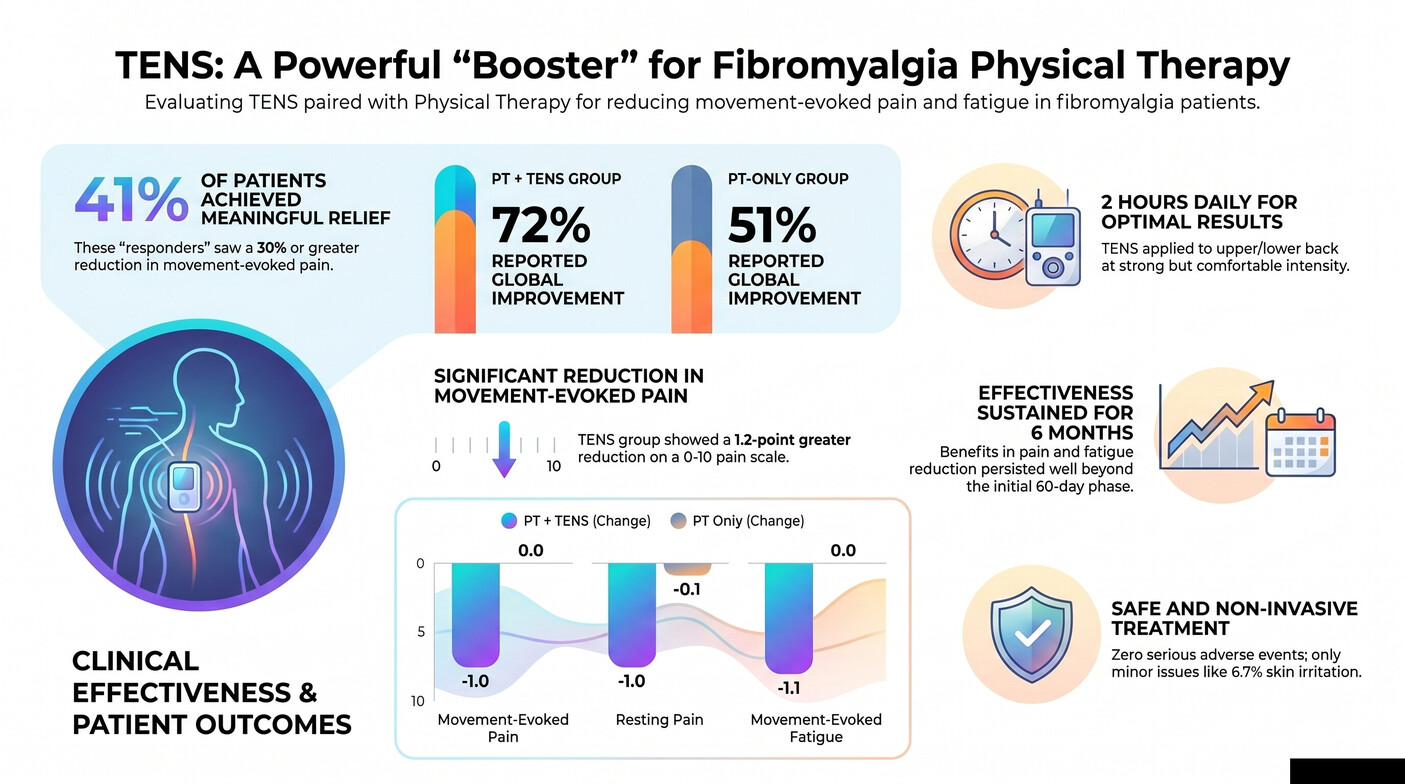
The results of the trial were striking. Participants were divided into a standard physical therapy group (PT-only) and a group combining therapy with TENS (PT-TENS). By the 60-day primary endpoint, the PT-TENS group reported significantly lower movement-evoked pain, showing a 1.2-point reduction on a 10-point scale compared to the PT-only group.
The most persuasive data, however, lies in the "responder analysis." This looks at how many individuals achieved a clinically meaningful change—defined as a 30% or greater reduction in movement-evoked pain. A remarkable 41% of those using TENS reached this threshold, compared to a mere 13% in the PT-only group.
The benefits also cascaded into other areas of life. The TENS group experienced:
- Significant reduction in resting pain.
- Lowered levels of both movement-evoked and resting fatigue.
- Improved "Patient Global Impression of Change."
- Reduced overall disease impact, as measured by FIQR scores.
5. The Dose-Response Secret: Consistency is Key
TENS is not a "magic wand" for instant relief; it is a tool that requires consistency. Researchers identified a clear "dose-response effect," noting that the greatest pain reductions occurred in those who used the device regularly during the first 60 days.
The "adequate dose" identified in the trial was at least 8 sessions per month for a total of 1600 minutes. For the average user, this synthesizes to roughly 50–55 minutes of daily use. To achieve the best results, electrodes were placed on the upper and lower back, and the device was used during activity. The sensation should be distinct but never painful. As the trial instructions noted, the device should be set to:
"parameters of modulating frequency of 2 to 125 Hz... at a strong but comfortable intensity."
6. Long-Term Benefits without the Long-Term Risks
Sustainability is the greatest challenge in chronic pain. The FM-TIPS data shows that TENS is not just a short-term fix; effectiveness was sustained for the full 6-month study duration. By the end, 81% of participants still found TENS helpful. Interestingly, even the participants in the PT-only group who were eventually given TENS during an "extension phase" (days 60–180) saw similar improvements, proving that the benefits are accessible even if the treatment is started later in the recovery process.
Safety also sets TENS apart from specialized pharmacological options. There were no serious adverse events reported. Minor issues were limited to skin irritation (6.7%) or itchiness (6.1%) at the electrode site. As an inexpensive, non-pharmacological, and readily available tool, TENS offers a way to manage symptoms without the systemic risks or costs associated with heavy medications.
7. The Future of Fibromyalgia Management: Conclusion
The FM-TIPS study represents a paradigm shift in how we approach fibromyalgia. By integrating TENS into a multidisciplinary approach, we finally provide patients with a self-management tool that targets the specific movement-evoked pain that has historically acted as a barrier to health.
This research effectively debunks the "no pain, no gain" approach to chronic pain recovery. It proves that for the fibromyalgia patient, comfort is not a luxury—it is a clinical requirement for progress. By lowering the volume of pain signals during activity, TENS acts as the missing bridge that allows the body to finally reap the rewards of movement.
As we rethink recovery, we must ask: how much more could patients achieve if we focused on making movement feel safe again? For the fibromyalgia community, the answer may finally be found in the "strong but comfortable" pulse of TENS.